|
|||||||||
|
|
|||||||||
       |
Feature Articles: Creating New Services with corevo®―NTT Group’s Artificial Intelligence Technology Vol. 15, No. 8, pp. 41–46, Aug. 2017. https://doi.org/10.53829/ntr201708fa7 Predicting Patients’ Treatment Behavior by Medical Data Analysis Using Machine Learning TechniqueAbstractThe analysis of medical information including electronic health records and medical image data using artificial intelligence (AI) has been an active area of research in recent years. The objective is to develop a means of supporting decision-making about treatment and medicine prescription by medical doctors. NTT has also been designing an AI for supporting diabetes treatment in collaboration with the University of Tokyo Hospital. We introduce here our machine-learning based technique to predict missed scheduled clinical appointments, which are likely to trigger treatment discontinuation by patients with diabetes. Keywords: diabetes, treatment discontinuation, machine learning
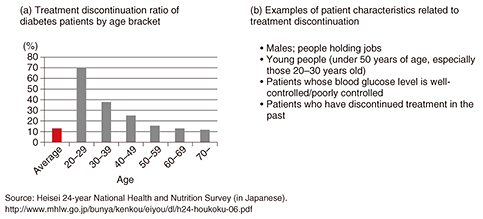
1. Treatment discontinuation in diabetes treatmentThe number of diabetes patients has been gradually increasing throughout the world. There are now over 3 million diabetic patients in Japan and approximately 380 million worldwide. Diabetes progression causes complicating diseases including diabetes retinopathy and nephropathy and results in a reduction in the quality of life and an increase in medical costs. Thus, it is vital for diabetic patients to begin medical treatment early and keep their regular hospital appointments to control their blood glucose level. However, in Japan, about 10% of diabetic patients discontinue treatment and return to the hospital after diabetes progression. This is one of the major problems in diabetic care (Fig. 1(a)). Researchers working to solve this problem have been studying the factors related to treatment discontinuation and have classified diabetic patients into two groups: those continuing and those discontinuing treatment. Multifactorial data were used to identify the differences between the two groups as risk factors by testing their statistical significance. Factors such as being male or holding a job proved to be high risks for treatment discontinuation [1] (Fig. 1(b)).
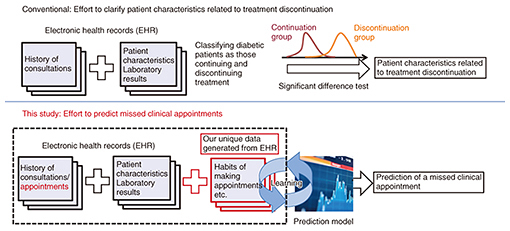
There are various factors related to treatment discontinuation, and it is therefore quite difficult for diabetes specialists to identify the patients who need a higher level of support. Therefore, NTT has been collaborating with the University of Tokyo Hospital in designing a prediction model that can predict treatment discontinuation at an individual level (Fig. 2). We designed the model to have features generated by a machine-learning technique that NTT developed and by applying knowledge of medical data analysis and the clinical experience of staff at the University of Tokyo Hospital [2].
2. Design of prediction model of treatment discontinuationWe focused our efforts on designing a model to predict a missed clinical appointment (MA) that can be a trigger for treatment discontinuation in order to identify the diabetic patients who require stronger support. We designed a logistic regression model that predicts a class y from a feature vector x of a patient’s target appointment, with y representing a clinical appointment missed (y = +1) or kept (y = –1) and x generated from the patient’s electronic health record (EHR), representing the time from the initial visit to just before the target appointment. We modeled the probability of an appointment with x attributed to y with a logistic regression,
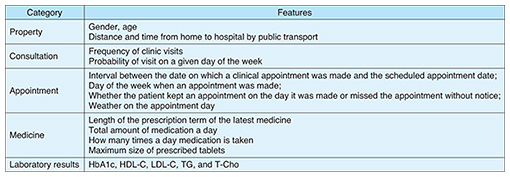
When the training data size N is smaller than the dimension of feature vectors, or a training data sampling is biased, maximum-likelihood estimation often overfits a logistic regression model into the training data, leading the model to classify many appointments inaccurately. Thus, we used an L2-norm regularization method to mitigate overfitting and improve the model’s generalizability. 3. Feature designTo obtain a prediction model with higher accuracy, we designed features using the knowledge of diabetes specialists, patients’ opinions, and the results of our behavior analysis. We designed two types of features: one that was automatically generated from EHR (X1 group, n = 29,025), and another that could be related to treatment discontinuation. Examples of the X1 group are listed in Table 1. These features concern the diagnosis and treatment department that each patient visited before the clinic appointment day, the name of their disease and the prescribed medication, the length of the prescription term (number of weeks, months, etc.), surgical procedures, and exams.
Examples of the X2 group are listed in Table 2. We designed these features based on patients’ behavior. Thus, the behavior characteristics and environmental factors of each patient weight the MA. For example, we included the day of the week and the weather on the day of a clinical appointment, and the pill size of the prescribed medication. We also referred to interviews with specialists and patients. A diabetes specialist explained that with patients who often forget to take their medication, the specialist monitored compliance by comparing the intervals between scheduled clinical appointments, the length of the prescription term, and the amount of medication the patient still had, so we incorporated the calculation as a check on compliance.
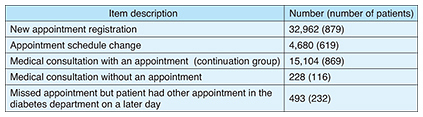
A diabetic patient told us that the accumulated experience with medical treatment in general stimulated his motivation to continue diabetes treatments. Thus, we used the history of clinic visits and the number of diagnosed diseases. We referred to databases maintained by the Japan Meteorological Agency and the Pharmaceuticals and Medical Devices Agency to respectively find weather information and the size of prescribed medication. In addition, we used gender, age, distance from home to hospital, and travel time, which previous research had identified as factors related to treatment discontinuation. 4. Evaluation of prediction performanceAll prediction experiments were performed using records from the University of Tokyo Hospital, which included the history of 16,026 clinical appointments scheduled by 879 patients whose initial clinical visit had been made after January 1, 2004, who had diagnostic codes indicative of diabetes, and whose HbA1c had been tested within three months after their initial visit. The records were dated between April 1, 2011 and June 30, 2014. We used the data to predict MAs in appointments. The actual number of missed appointments and kept appointments was 922 and 15,104, as indicated in Table 3.
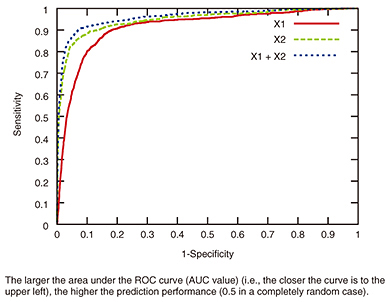
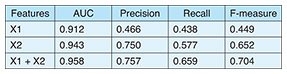
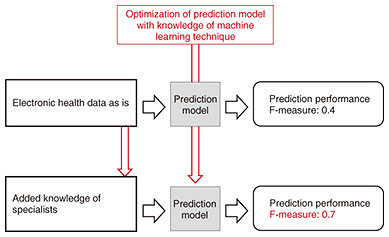
We examined the difference in prediction performance between models by using the X1, X2, and X1 + X2 groups with a receiver operating curve (ROC) (Fig. 3). The model compared the area under the curve (AUC) values between them. An AUC value of 0.943 was obtained for the X2 group, leading to a prediction of MAs with higher accuracy than for the X1 group (AUC = 0.912). The AUC for both the X1 and X2 groups (AUC = 0.958) yielded even greater accuracy, as indicated in Table 4. An AUC value of more than 0.9 generally means excellent discrimination in such performance evaluations. We can therefore say that our model can predict MAs with high accuracy and help to identify the patients needing stronger support to maintain treatment; it also helps to determine when doctors should support them. The precision, recall, and F-measure of the model when using both X1 and X2 groups were 0.757, 0.659, and 0.704, respectively, although the F-measure was 0.449 when using only the X1 group, as indicated in Table 4. We can also say that we succeeded in obtaining a model with high prediction performance by designing features related to treatment behaviors. The relationship between input data and prediction performance is shown in Fig. 4.
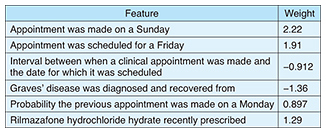
5. Features contributing to MA predictionWe compared the weights of features used in this study to investigate what the contributive features were for MA prediction. The contributive features are listed in Table 5. These features were given the largest absolute weight in our trained model and thus contributed strongly to MA prediction. We found that features related to when and how appointments were made, rather than to patients’ clinical condition, influenced the accuracy in predicting MAs. Some contributive features were, for example, “Appointment was made on Sunday,” “Appointment was scheduled on Friday,” and “Interval between when a clinical appointment was made and the date for which it was scheduled.” Of these, the last characteristic amount is a negative value, which means that the shorter the interval between when a clinical appointment was made and the date for which it was scheduled, the more likely a missed clinical appointment will occur. These features found by our model were valued by a diabetes specialist because it is generally difficult for medical doctors to find them.
We believe that our model will be a powerful tool to improve patients’ medical condition since it makes it possible to identify patients who need more support, to assess when they should be strongly supported, and to control the strength of intervention with each patient. 6. Future developmentWe designed a model that can predict with high accuracy when a diabetic patient is likely to miss a scheduled hospital appointment, possibly leading to discontinuation of treatment. This is the first study utilizing machine learning to design this kind of model. Various techniques that can provide information appropriate to humans have been proposed as recommendation techniques in the machine learning field. We plan to continue studying machine learning in order to develop solutions to prevent treatment discontinuation. One of our collaborators who has been studying telemedicine demonstrated that patients’ behavior related to their meals can be improved if they are given feedback on their lifestyle habits based on the data [3]. Thus, we believe that giving patients feedback on the confirmation of appointments will be one of the solutions to motivate patients who may potentially discontinue treatment. The standards for EHR and SS-MIX2 (Standardized Structured Medical Information Exchange) are now being widely implemented, and an environment for handling massive amounts of clinical data is being prepared, so we will focus our efforts on improving our prediction model while utilizing these advances. References
|
||||||||